



Intro
This blog post covers identifying the need for MTP, MTP protocol, goals of therapy, evidence behind MTP, adjuncts to MTP, and newer testing for coagulopathy. There is also a review of blood transfusion reactions.
Identifying Need for MTP

MTP, think TXA!
Massive Transfusion Protocol (MTP) is an important step in most trauma protocols. By recognizing the severity of injury and intervening quickly by giving blood products upfront, MTP has been shown to decrease ICU length of stay, decrease ventilator length of use, decrease mortality rates, and has been shown to decrease the number of blood products needed over the entire length of stay.
Just a quick refresher on our ABCDEFGHI mnemonic for any trauma that walks through the door.

After completing the primary survey and obtaining history, we need to decide if patient meets criteria for MTP. There are two scoring systems for evaluating the need for MTP as well as one scoring system for pediatrics. Essentially, these tools state the obvious that if there is blunt or penetrating trauma in patients with hypotension and tachycardia, then you should be leaning towards MTP.
- ABC Score >2
- Each of the following scores 1 point: penetrating mechanism, SBP<90, HR>120, positive FAST. If patient meets 2 of these factors, then MTP should be considered
- Shock Index (SI) >1
- HR divided by SBP equals shock index (HR/SBP=SI) Essentially if your HR becomes greater than your SBP, then this is bad (e.g. HR 120 and SBP 100 is bad, with SI=1.2)
- This was found to be more sensitive in predicting need for MTP than ABC score but not validated in kids
- SIPA (Shock Index Pediatric Adjusted)
- Available on MDCalc and takes into account patient’s age as this will impact their relative scoring based on age-adjusted HR and BP normal ranges

What is MTP?
MTP is defined as either:
- 4 Units of PRBC in <4 hours with ongoing losses
- >10 Units of PRBC within 24 hours
The goal of MTP is to rapidly provide blood products while also preventing the “lethal triad” of acidosis, hypothermia, and coagulopathy that prolongs hemorrhage.

Source: rk.md
MTP Protocol
Most protocols start with 2 U PRBC, 2 U FFP, and 2 U plts upfront once MTP is activated. The patient is closely monitored thereafter, and if more blood products are needed they are given in a 1:1:1 fashion.
***Of note, platelets come in a “pack” which typically contains 5-6 U of plts depending on the institution. This is important to be aware of when calculating the number of blood products given
***Also MTP protocols are institution derived, therefore, there can be slight variation in the 1:1:1 ratio, however, they are typically minor alterations
Goals of MTP Therapy
Blood Pressure (combatting hemorrhagic shock)
- Typically a strategy of permissive hypotension (80-100 SBP) is employed. However, in TBI patients a higher BP range is often targeted
- Hgb targets are often not employed in MTP protocols as they are less reliable during acute hemorrhage either being falsely elevated (“behind the curve” of hemorrhage) or falsely decreased (dilutional component).
Temperature
- Goal Temp >35C
- Hypothermia is a large issue in trauma and MTP patients. It is multifactorial from exposure (wet clothes off, warm blankets on), loss of blood products (lose a lot of heat from hemorrhage), infusion of cold IVF and blood products (can use fluid warmers).
- Hypothermia further contributes to the “Lethal Triad” as decreases function of clotting factors and furthers metabolic acidosis.
- Often central temperature is used (ETT, foley, rectal) for accurate temperature gaging
pH (combatting acidosis)
- Goal pH>7.20, base excess <-6, lactate <4
- Acidosis is caused by hypoperfusion from hemorrhagic shock as well as contribution from IVF resuscitation, which is why some trauma protocols limit amount of IVF to 0-2 L in total for the resuscitation. Recall that NS has pH ~5.5 and LR has pH ~6.5. Of note, PRBCs are also mildly acidic with pH 6.8-7.0 (depending on age of unit).
- Acidosis leads to platelet and coagulation factor disruption.
Coagulopathy
- Goal of Plts >50,000, INR<1.5, fibrinogen >150-200 mg/dL
- Caused by direct exsanguination/loss of plts and clotting factors as well as consumptive process as body tries to achieve hemostasis. Also large dilutional component as body shifts extravascular fluid to intravascular (lowering concentration of clotting factors) to maintain BP. Also iatrogenic dilution from IVF resuscitation.
- Of note, FFP has intrinsic INR ~1.4, therefore, it is not possible to lower INR to value <1.4 with FFP
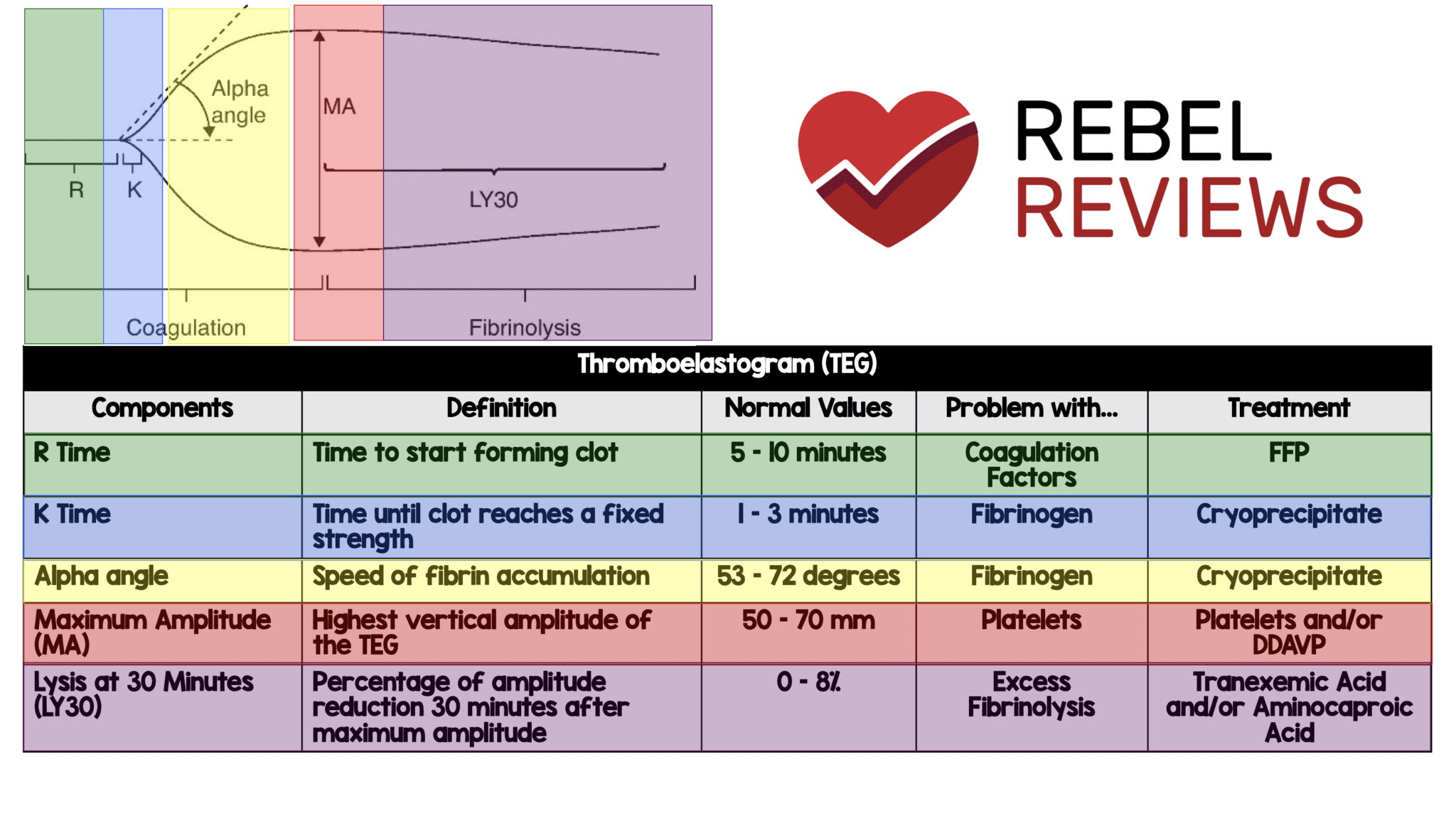
Measuring Coagulopathy in Traumas (TEG)
This is an area of change at many trauma institutions. Standard coagulation tests such as INR/PT, PTT, platelet count, and fibrinogen levels often take 30-60 minutes and are performed in the laboratory. They are also limited because they purely test the amount of clotting factors present, which may not be a true indication of their functional level. As we mentioned above, several areas impact coagulopathy (acidosis, hypothermia), and although, the amount of clotting factors can be normal, their function may be abnormal.
One tool that is becoming popular is TEG (thromboelastography). TEG uses a sample of blood and then performs in-time testing of the blood’s ability to clot (takes 20-30 minutes). It uses a cylinder with a rotating pin and light to measure the refraction of the blood to test the time of clot formation, strength of clot, as well as level of fibrinolysis. The results are presented in a graph with 5 different parameters reflected (link to below graph if blurry). Based on below measurements, specific blood products can be given to combat the coagulopathy. If you want more practice on interpretation of TEG, I thought this YouTube video was helpful (30 minute video (even better on 1.5x speed), he starts giving graph examples at 9:30 minutes. Prior to this is an intro on TEG).
{kind=link}

Calcium
- Goal iCal >1.1 mmol/L
- Hypocalcemia is caused by citrate that is present in PRBCs which can bind with plasma calcium causing hypocalcemia
- Hypocalcemia can lead to negative cardiac ionotropy further contributing to hypotension
Potassium
- K<5.0
- Hyperkalemia is most often from the K present in PRBCs. Of note, “older” Units of PRBCs will have more potassium than newer units as more K is released as the RBCs degrade with age. Acidosis also can lead to cellular exchange with H+/K+ transporters further contributing to hyperkalemia.
Typical Blood Products (ingredients) of MTP
The reason for the 1:1:1 (FFP:plts:RBC) ratio of blood products is from the PROPPR Trial (2015), which compared 1:1:1 ratio vs. 1:1:2 ratio (meaning 2nd group received extra units PRBC). This was a non-inferiority study, however, it also showed increased hemostasis at 24 hours in the 1:1:1 ratio.
- PRBC
- Most PRBC have shelf life of 42 days which is achieved via addition of anticoagulants and citrate.
- ~300 mL/unit
- Each unit will raise Hgb by 1 g/dL on average
- FFP
- Must be thawed prior to administration (can take up to 30 minutes)
- contains high levels of factors II, V, VII, IX, and XI
- Must be ABO compatible
- 250-300 mL/unit
- Plts
- As we hammered home, platelets are typically provided in single “pack” which has 5-6 U
- 1 pack (which is 5-6 U plts) is ~300cc/bag
- Cryoprecipitate
- contains fibrinogen, vWF, Factor 8, Factor 13, fibronectin
- 10-12 mL/unit. Often given as 10 U so ~100cc/infusion
- Each unit will increase fibrinogen level by 7-10 mg/dL
- TXA
- Antifibrinolytic agent (stabilizes formed clots) and inhibits plasminogen activation
- typical dose is 1 gram over 10 minutes (slow IV push) followed by 1 gram over 8 hours (mixed in 50 mL of NS)
- I love TXA. It has tons of uses and several studies being published on its role in all purpose bleeding. We could probably do a whole blog post on just TXA, but why do that when REBELEM just made an amazing all encompassing post on TXA one month ago
-
- TXA improves survival at 4 weeks when given <3 hours after time of injury. No evidence of increase in vascular occlusive events
- Drawbacks: randomization was not ideal, no MTPs, no decrease in blood use, half the patients did not require any blood
- Be on the lookout for CRASH 3 Trial which just ended enrollment in Jan 2019 and should have published data later in the year.
- MATTERS from the clever acronym “Military Application of Tranexamic Acid in Trauma Emergency Resuscitation” assessed 896 soldiers treated at a single hospital in Southern Afghanistan who received at least 1 U PRBC from trauma
- Showed mortality risk reduction 7.6%, improved coagulopathy measures, and improved rates of survival in TXA group. TXA also showed increased rate of VTE, however, no deaths occurred secondary to this complication.
- Drawbacks: single center military hospital in a very young cohort (average age 24), no data on timing of TXA administration, these patients also received cryoprecipitate

Transfusion Reactions
Anytime we’re giving blood products, we need to be vigilant for transfusion-related complications. They are listed below in time to onset of reaction
Anaphylaxis (seconds to minutes)
- caused by patient’s IgA antibodies. Therefore, this risk is greater in patients with IgA-deficiency because they have anti-IgA antibodies that will attack donor’s blood. If this reaction occurs, patients should be tested for IgA deficiency
- If future transfusions are needed, patient should receive IgA-deficient blood
- Tx: stop transfusion, IM epinephrine, supportive care
Acute Hemolytic (minutes to 1 hour)
- due to ABO incompatibility often from infusion of mismatched donor blood
- presents as fever, chills, flank pain, hemoglobinuria. This can progress to renal failure in severe cases (due to immune complex deposition) and DIC
- Dx: Coombs test positive, hemoglobinuria, repeat type and cross and double check donor blood
- Tx: stop transfusion, IVF, and supportive care
Febrile Non-hemolytic (1-6 hours)
- Most common reaction. Occurs from residual plasma and/or leukocyte debris remaining in PRBC. During blood storage, these remaining leukocyte debris release cytokines which can cause transient fevers, chills, and malaise. There will be no evidence of hemolysis on labs.
- We prevent this reaction by using “Leukocyte-reduced blood products”
- Tx: stop transfusion to exclude other serious reactions, Tylenol for fever, supportive care
Urticarial/Allergic (2-3 hours of transfusion)
- Caused by patient’s IgE antibodies that lead to mast cell activation leading to urticaria, flushing, edema, and pruritus
- Tx: benadryl, pepcid, prednisone
TRALI (1-6 hours)
- “Transfusion Related Acute Lung Injury.” 1 in 12,000 transfusion. Although rare, most common cause of death from transfusion. Thought to be from acute neutrophilic response that leads to pulmonary endothelial damage and massive capillary leak leading to ARDS-like syndrome.
- Looks and acts like ARDS. Characterized by hypoxemia (O2<90% on room air) and bilateral pulmonary infiltrates presenting within 6 hours of transfusion. May also have fever, hypotension, and tachycardia
- Tx: stop transfusion, close respiratory monitoring as may require NIV or intubation. Vent settings similar to ARDS with low TV and higher PEEP
Delayed Hemolytic (2-10 days)
- Mild fever and mild hemolytic anemia. Caused by anamnestic antibody response to antigen (antibody is undetectable prior to transfusion but rapidly reappears following transfusion due to exposure from antigen in PRBC)
- Dx: positive direct Coombs Test with positive new antibody screen on T+S.
TACO
- “Transfusion-Associated Circulatory Overload.” Occurs from volume overload from high amounts of blood products. Looks and act like heart failure
Final Note
“A pint of sweat will save a gallon blood” –George S. Patton
W