Heres the no frills details behind ITP and TTP. Your board scores can thank me later.
Idiopathic Thrombocytopenic Purpura (ITP)
ITP is an autoimmune reaction where your B cells have done messed up and make antibodies to antigens on your platelets. Patients will typically come in with petechiae or purpura in dependent portions of the body. They may even have epistaxis. Very rarely will they have severe hemorrhage. Also, they probably look like a child; ITP is more common in the pediatric population.
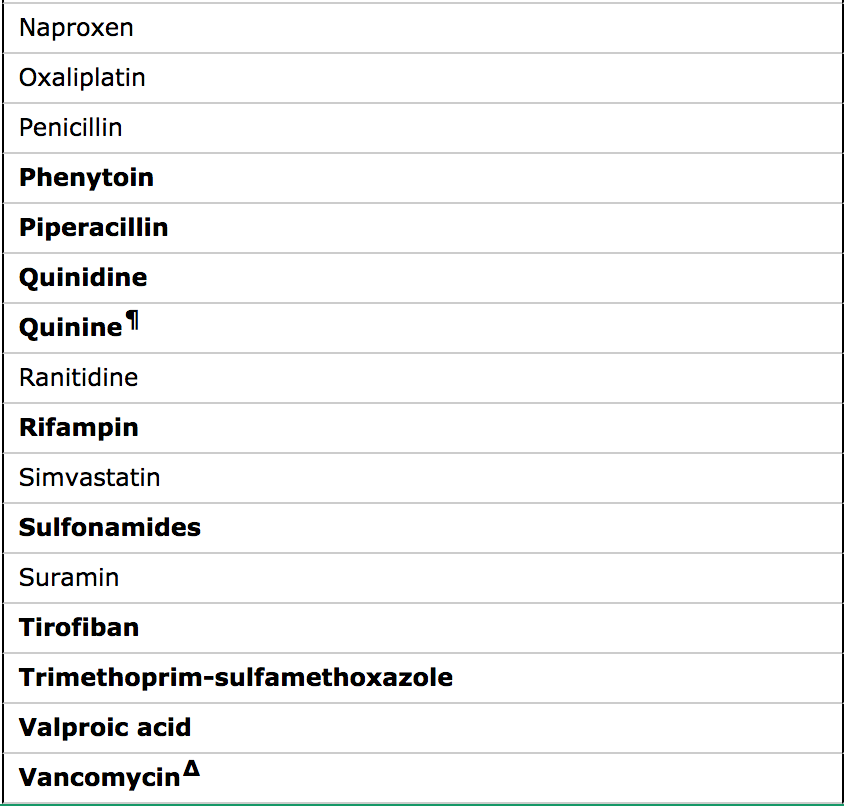
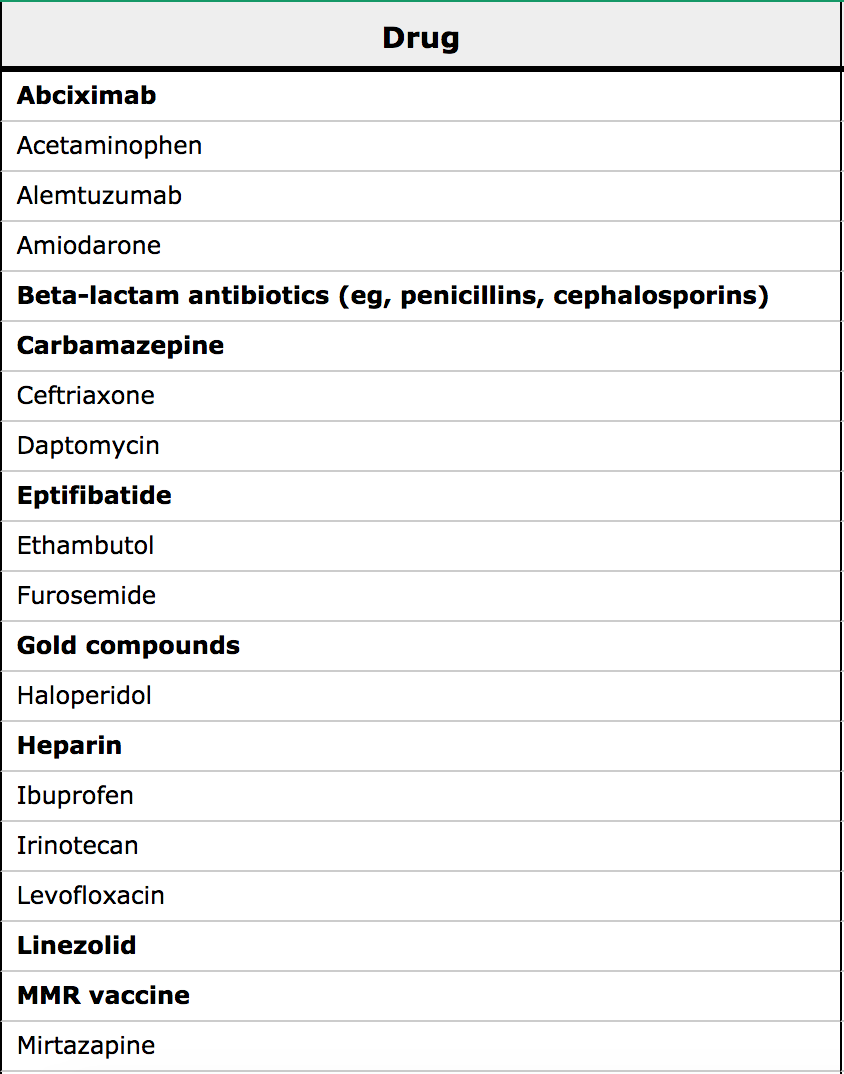
However, even if your patient meets the bill entirely: this is a diagnosis of exclusion. They need to have isolated thrombocytopenia (no other CBC abnormalities.) A ton of medications can cause thrombocytopenia, so go through an intensive medication review with your patient, even over the counter medications. Also, check that pregnancy test, and look to see if they have known causes of secondary ITP: HIV, HepC, Lupus, CLL.
If you’ve excluded it all and decide that this patient has ITP: it would be nice for them to have at least 20, 000 platelets. But don’t give them a platelet transfusion… those antibodies we talked about will just keep attacking. Instead give them high dose glucocorticoid and admit them for IVIG.
Thrombotic Thrombocytopenic Purpura (TTP)
TTP is the one with the ADAMTS13 deficiency. Usually little AdamT is a von Willibrand Factor (vWF) protease, so when people are deficient they get vWF mutimers that cause tons of platelets to aggregate. They become thrombocytopenic because their platelets are being used up in these clumps AND these clumps then hemolyze RBC’s as they try to squeeze past. Just little RBC’s trying to get to work and getting sliced by clot traffic jams.
The other word you associate with TTP from your board days? FAT RN: Fever, Anemia, Thrombocytopenia, Renal failure, Neuro symptoms. You will see other lab changes: mainly from the microangiopathic hemolytic anemia: elevated LDH, low haptoglobin, elevated indirect bilirubin. BUT you will always have the anemia and the thrombocytopenia.
Keep in mind this is a rare disease, so keep your differential broad. Don’t forget our other platelet clotting, petechiae forming friend DIC. So go ahead and add on those DIC labs: PT, aPTT, DDimer and Fibrinogen. And if you need even further proof that its TTP you can use the Plasmic score.

Treatment for TTP is Plasma exchange therapy, if this is not available at your hospital- FFP can provide temporary benefit. However, don’t give patients platelets unless they have uncontrollable, life-threatening bleeding. Otherwise those little guys will just go off to aggregate into more schistocyte-forming traffic jams.
In Conclusion:
- ITP: less sick, no hemolytic anemia
- TTP: more sick, hemolytic anemia +/- (FAT RN)
- HUS: more renal- less neuro involvement, recent hx of diarrhea
- DIC: more bleeding, elevated coags and DDimer, low fibrinogen