Here’s a summary of the more common forearm fractures and what to do about them.
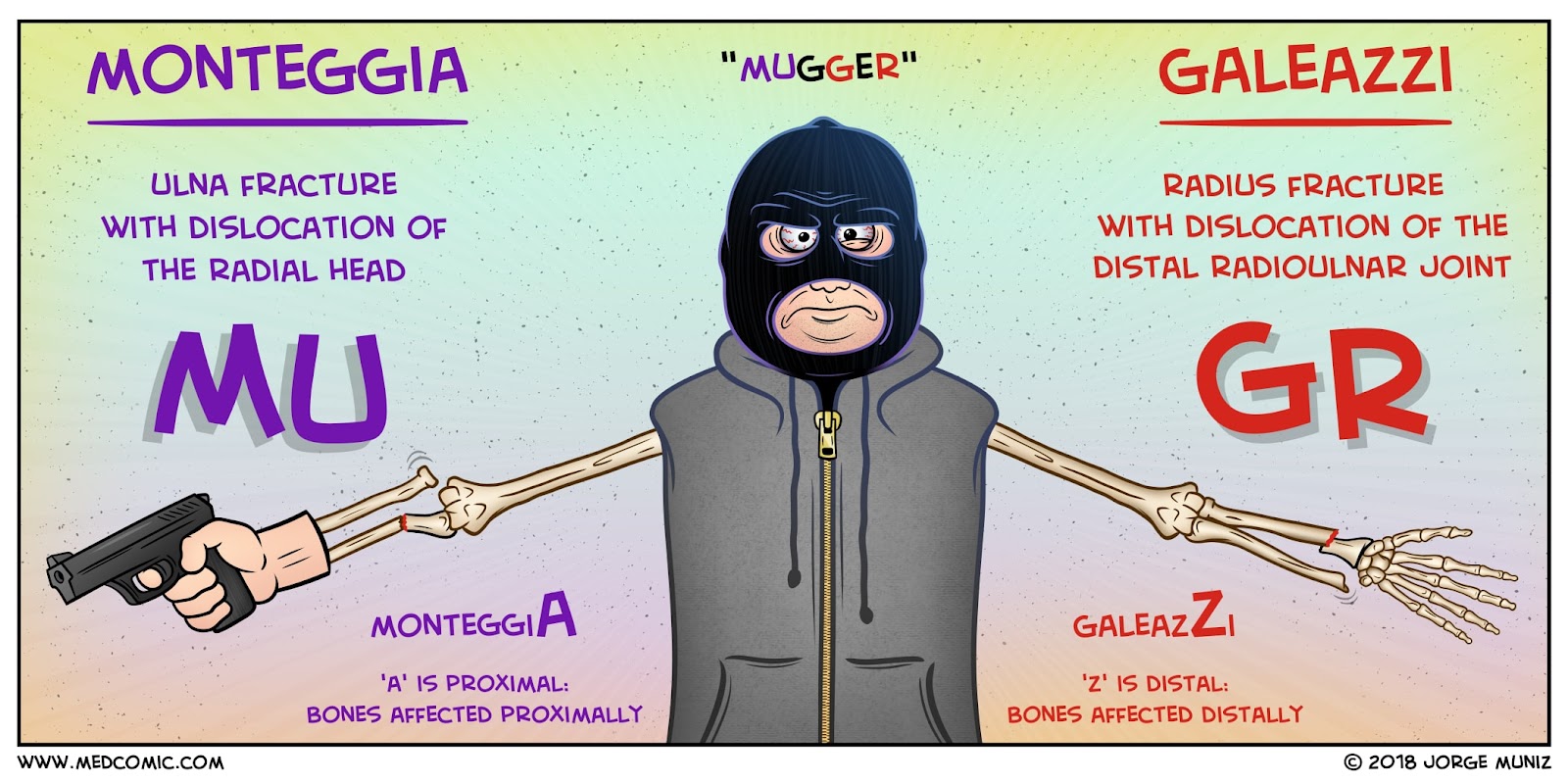
Galeazzi v. Monteggia
For both of these diagnoses, the patient will likely tell a story of a FOOSH while in pronation. You’re also gonna place both of these in long arm splints in supination in the ED. But here’s the difference:
Galeazzi
Though a distal radial fracture may be obvious with deformity, make sure to take a look for disruption of the distal radio-ulnar joint (DRUJ) on XRays. Though we typically preach this to be widening of the DRUJ space (>2mm), Galeazzi also defined disruption to include a fracture at the base of the ulnar styloid process or greater than 5 mm shortening of the radius relative to the distal ulnar. So what’s the big deal you ask? You don’t splint these like you would a simple radial fracture. These have really high risk of complications with cast immobilization so you want to let your Orthopod know sooner rather than later so they can ORIF these bad boys. Meanwhile, reduce the radial fracture as needed and place patient in a long arm splint in supination.

Monteggia
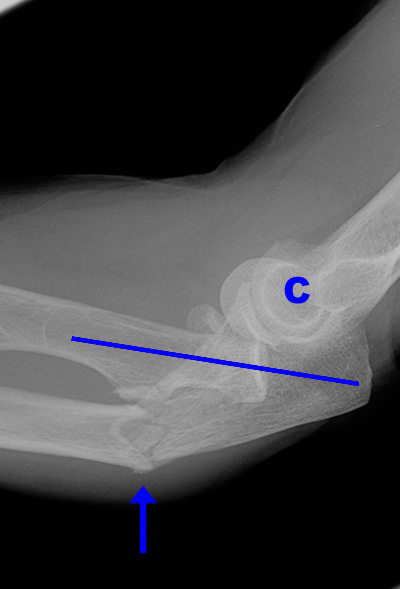
Compared to the Galeazzi this is more common in kiddos. A Monteggia fracture is any ulnar fracture associated with radial head dislocation. Make sure you do a complete neurovascular exam as radial nerve deficits are common (up to 17%!) Sooo look for wrist drop, dorsal hand sensation lost or most commonly finger extension weakness (posterior interosseous branch.) Again, especially if this is in an adult- they are likely to need surgical intervention, so get Ortho involved early. Otherwise, reduce the radial head dislocation and place patient in long arm splint in supination.
Colles v. Smith v. Barton
These are three more don’t miss diagnoses associated with falling on hands. Key point: Colles will be a typicall FOOSH, Smith will be a history of a flexed hand.. a FOFH, if you will.
Colles
The XRays will be evident for dorsal displacement of the distal radius. Also described as the dinner fork deformity, reduce the fracture and place in a sugar tong splint. Most likely patient will be able to be managed non-operatively but have them follow up relatively soon with ortho, unstable Colles are likely to lose the reduction, have instability or develop early onset of arthritic symptoms.
Smith
Basically this is same, same but different. The radial fracture will include palmar displacement of the distal fragment. Reduce, place in long arm or sugar tong and give them prompt ortho or hand specialist follow up.
Be careful though, these might marketed as “Reverse Colles” but these are much more likely to be unstable or have nerve/ligamentous injuries. We might be doing the same thing in the ED- but let your patient know- there is a high chance they may need surgical intervention.

Barton
In either case of the above be sure to assess for carpal displacement. This then changes the diagnoses from Colles or Smith to a Barton’s fracture. Most require surgical management, so give them prompt follow up. Cast them in double sugar tong splint.
Nightstick Fracture
So this one I actually knew about before I came into medicine – healed isolated ulnar fractures are some of the most commonly found bone trauma on archeological digs showing evidence of interpersonal violence. Woot for the social sciences! Sad woot for humans being so predictable.
Basically when someone is coming at you with a hard object (let’s say a night stick, for instance) your natural instinct is to hold your arm up to block the blow. If struck hard enough this can fracture the ulnar shaft. Since we aren’t way back in the stone age- place these patients in a long arm cast and have them follow up with Ortho. Most likely they will be placed in a cast for 6-8 weeks.
Conclusion:
Watch out for the Mighty FOOSH people. I’ve talked about it’s effects on the forearm but don’t forget to evaluate for other wrist or elbow complications. Touch that snuffbox. Do it.
Remember, despite the fracture or what I said above- any time the fracture is open or there is evidence of neuro-vascular compromise urgent evaluation by an orthopedic surgeon is required. So make sure your exam is thorough before you run off to get supplies.
