Here’s some how to’s when it comes to burns. First off- do your ABCs. Get your history from the patient, from family, from EMS. You need to figure out the mechanism of this burn. Was this an explosion? You may need to worry about associated injuries. Was this inside? You may need to worry about toxic gases.
In your exam, we all know to look for signs of smoke inhalation. These patient’s may need a tube as their airway reacts by being a bit of a drama queen and swelling closed, because that’s exactly what this poor patient needs. On top of this, the smoke may cause laryngospasm, so if the patient could tolerate it, try to give them some albuterol. But remember this laryngospasm may make passing that tube pretty difficult, so have surgical airway supplies on hand. It may behoove you to mark up your incision site at this time too, just in case.
The other big test question exam finding? Total Body Surface Area (TBSA) . Use the rule of nines. Don’t forget that babies are adorable and have giant heads- so their percentages are different. If, because we practice in real life and not in boards questions, the burns are splotchy and do not take up the entire 36% of the torso.
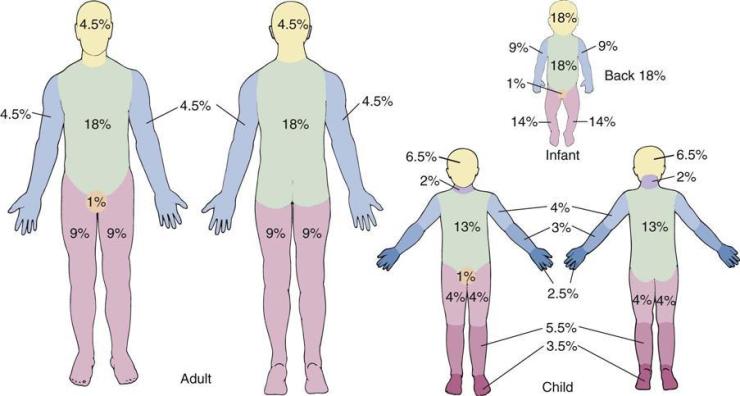
You can use the size of the patient’s palm to estimate percent. One palm sized splotch would be about 1%. Be sure you use the patient’s palm. Don’t underestimate their TBSA just because your hands are the size of a dinner plate.
Then use the TBSA to decipher how much fluid to give (Parkland formula) AND to decide who needs to go to a burn center.
Burn Classification
Since we’re hoity-toity doctors we wanted to further separate our language from the lay person and decided that the degree system doesn’t work for us. So let’s talk about how to talk about burns.
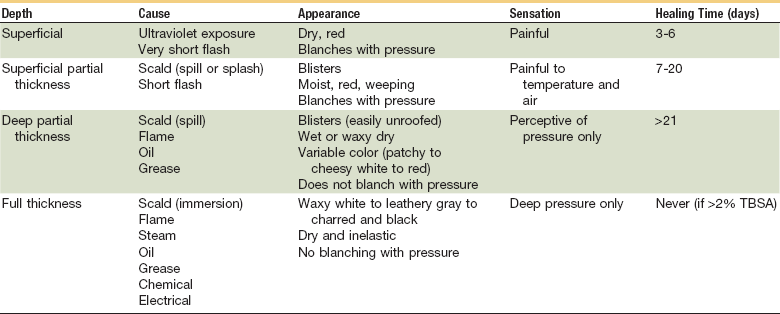
To make it quick and dirty for you- here’s a table that I found on the google.
Superficial Burns
These present as a blanching, dry, red discoloration of the skin. These burns are painful. Think of a really bad sun burn. Basically you rub some lotion on these patients, and suggest they try aloe. You can ignore all the other treatments I talk about below. These burns should heal in about 3-6 days, so let them know they’ll be feeling kinda miserable for a hot sec.
Superficial Partial Thickness
These burns typically occur from a splash or a flash burn. The burn itself is blistered, pink, moist, and is painful. These patients may need a burn center if they have a partial burn >10% TBSA or a burn to their important pieces (face, hands, genitalia, etc.)
Deep Partial Thickness
As is obvious by the name, these burns extend deeper into the skin layers: all the way through the dermis.But basically these can present as any variation between superficial partial and full. They can be any color, wet or dry. They can have blisters. But they aren’t superficial partial because they do not blanch. And they aren’t full thickness because there are no eschars. Use the same decision process as superficial partial thickness to decide who to send to a burn center.
Full thickness
No matter what, these patients need to go to a burn center. To try to prevent contractures, serious infections, death these patients are going to need debridement, excision, re-excisions, grafts and a whole lot of love and care by specialists.
ED Management
If you are shipping your patient off to a burn center, start them on fluids, monitor input with urine output (.5 ml/kg/hr,) attempt to keep them warm, intubate them if needed, throw in an NG ( if at >20% TBSA, patients are at risk for ileus) and place a foley. Get them out.
But it this is a patient with less than 10% TBSA and its not on a special bit (again face, hands, genitals, etc.) then we can do a little bit of our own burn care in the ED. Apply some silver sulfadiazine to the wound and cover with xeroform gauze. Tell them to change their dressing twice a day and follow up. If this is a pregnant lady or breast feeding, skip the sulfadiazine… it’s a category B drug with concern for kernicterus!
Even if this is a tiny burn, its gonna be a super painful healing process. Give them some opioids or consider a regional block if you’re admitting them.
Toxic gas inhalation
Think CO C O.
| Toxic Gas | Symptoms | Diagnosis | Treatment |
| Carbon Monoxide | Red skin Headache | Blood CO level | -Oxygen -Dive: to help prevent neuro symptoms IF + Pregnant + Blood levels >40% + Any neuro symptoms + Acidemia |
| Cyanide(from combustion of material containing Nitrogen(i.e. plastic, vinyl, wool) | Red skin possible | VBG with high O2 but lactate is also super high | – Cyano-kit Or – Cyanide antidote(don’t give sodium nitrate if significant burns bc it creates methemoglobim which they already have enough of) |
| Oxidizers | Blue Mild low O2 sats | Methemoglobin level-chocolate brown blood | – Methylene Blue |
Conclusion
Most burn patients will die from something other than their burn. Make sure you don’t miss anything else going on. Remember your math equations but don’t forget to do a thorough physical exam. Including the eyes!
Despite the classic boards question- call the Burn center before performing an escharotomy. That being said- if an intubated patient becomes difficult to bag or desats and nothing else comes up in your search for why, this patient may need chest or even a subdiaphragmatic transverse escharotomies. The latter especially in pediatric patient’s as they tend to belly breath.
All this being said- don’t forget about electrical and chemical burns. They’ve got their own presentations, secondary injuries and treatments that you can’t miss. If I had to summarize bits that I found important about these topics from our lecture it would be in these short kinda useless statements:
- Electrical – Get an EKG and full neuro exam. Some neuro findings may be transient. Muscle tetany can fracture bones and the burn may be more extensive than what is visible on the skin.
- Chemical – Bases are worse than acids, unless its HF because that shzz acts like a base AND eats up all the calcium. Decontaminate, Irrigate!
Please do a bit of your own googling or Tintinalli-ing or however you do-ing to study up on what makes these burns different and what to do about it!