Patients who have a history of IBD: chronic abdominal pain, diarrhea, fever, weightloss; coming into the emergency department for these same symptoms; how do we handle chronic disease in the emergency department?
ED Work up
First a review of the details shmetails:
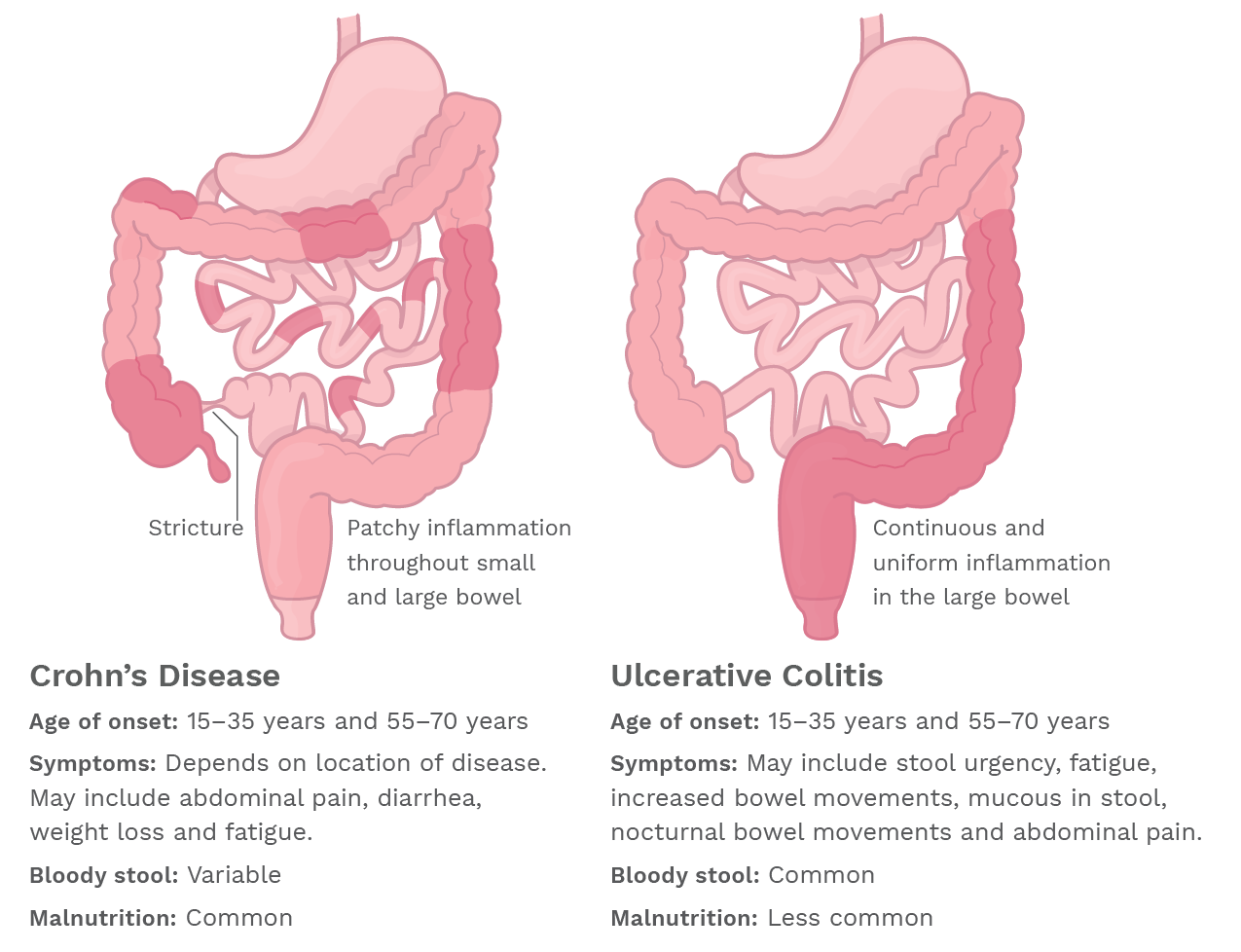
| Crohn’s | Ulcerative Colitis | |
| Transmural + skip lesions | Mucosal ulcerations + continuous | |
| Complications: | Obstruction Fistulas Intra-abdominal abscess Malignant Neoplasms | Toxic Megacolon GI hemorrhage Strictures Crypt Abscesses |
25% of UC patients will require a colectomy and 90% of CD patients patients will require at least one surgery for major complication in their lifetime. Most of these complications, especially the surgical emergencies, can be caught by a CT scan with IV contrast. But for the sake of their kidneys and the chance that they might start glowing at night – it is important to not scan them when it is most likely simply a flair of their chronic disease without complication. CT yield has been shown to be low in these patients. A recent study shows that though we’ve increased our scanning of these patients but that their admission rate has not changed… (Kerner et al) AKA we are scanning them and not finding anything. So how do we hone down who gets scanned?
If the patient is reporting simply worse pain, worse diarrhea – they likely do not need any imaging. If you are concerned for obstruction- maybe start with KUB first. If you are concerned for perianal/rectal disease- consider an endocavitary probe. Unfortunately, there are not any truly validated predictor scores for IBD. So we are up the canoe without an MDCalc tool. The important thing is to discuss with the patient their typical symptoms and what is different about THIS episode? Sure it very well could just be a flair- but you don’t want to miss some of those big scary complications up above. A trusty chart review may help you see what their unique disease pattern has been, but let’s keep a little faith in the patient and make sure you get details on their previous presentations and complications.
- Kerner C, Carey K, et.al. Clinical predictors of urgent findings on abdominopelvic CT in emergency department patients with Crohn’s disease. Inflamm Bowel Dis 2013: 1179-1185
Extra-intestinal Life forms
Don’t forget that both IBD’s can have manifestations outside the bowel. Including ocular, skin, cardiovascular, and other GI issues. So make sure you look to these for treatable complaints as well.

Patient’s with IBD (UC > Crohn’s) may develop Episcleritis or uveitis. The big difference is that Episcleritis will be localized to the epi-sclera and usually occur during an IBD flair. Go ahead and give them lubricating eye drops +/- some topical ‘roids.
For uveitis, often be a more long standing issue, bilaterally and diffuse; give them steroids and cycloplegics .
Cardiovascularly… these patient’s are at higher risk for basically any classic heart disease. If they don’t already- make sure they have cardiology follow up and try to convince them to lead that healthy diet and excercise lifestyle.
Patient’s may also develop cutaneous manifestations that often proceed an IBD flair. Pyoderma gangrenosum will need Derm to follow up. Erythema Nodosum will be more self limiting and can be discharged with steroids, NSAIDS and potassium. Since derm is such a toss up, I suggest you look these up to see a variety of possible skin changes.
Of course, other organs in the abdomen like to get their hands dirty too. Be aware of the higher risk for Portal vein thrombosis, pancreatitis, cholelithiasis, Primary biliary cirrhosis, and Primary Sclerosing Cholangitis.
Pain Control

These patient’s are in pain, they look like they are in pain. But try not to give them opioids.
Opioids actually worsen the pain in the long run by increasing the inflammatory state. Their GI doctors aren’t giving it to them… so maybe we should try to avoid it as well. I’m not saying to not give them anything. Help with their flairs with some IV steroids to decrease the inflammatory state, consider antibiotics if possible infectious etiology. And consider ketamine!
.3mg/kg Ketamine in a 1Li NS bag + a small dose of Benzos has been shown to have some effectiveness for pain control in these patients. You’re gonna be giving them fluids for their diarrhea anyways… why not try something other than narcotics?
Pearls
- Consider IBD as a new dx in young adult patient’s that continue to return to the ED for abd pain.
- Fever may just be from the flair, not every fever needs antibiotics.
- Try ketamine!
- Acutely ill? Grab a quick XRay first – for rapid assessment for perf or toxic megacolon.
- UC is the one time you may tell your patient it is okay-ish to smoke – smoking is preventative in UC.. but waaaay worsens the flairs in Crohn’s.
Special Thanks to Dr. Dissanayake for the wonderful presentation on IBD!