Author: Dr. Catherine Buckley
Alright. LVADs. First thing is first- use a lifeline and phone a friend. Call the patient’s VAD coordinator. Patient may have a card that they are able to give you… but if the patient is otherwise incapacitated, look for a tag on their controller.

Vital-ing
Take a looksy at the image above. Basically this device works by sucking blood from the left ventricle and pumping it in one beautiful fluid movement to the Aorta. What’s that mean? Your patient may not have a pulse. So, instead use your stethoscope to listen over the heart for the reassuring whirr that shows that the pump is working. Adjust your assumption of this patient’s well being by taking in other clues: i.e. Mental status, pallor, the machine itself. Is the control unit flashing warning signs? You can still measure your patient’s blood pressure! But diastolic and systolic measurements require a pulse (remember learning how to take BP?) … so instead use a manual cuff and listen (with doppler, stethoscope, etc in the AC like the old days) for the pressure at which you begin to hear a beautiful, continuous hum. That, my friends, is your MAP. Now an A-line measured MAP will be more accurate but ain’t nobody got time for that… well until you do.
Meanwhile
You should be sending off labs – remember that these patients are super duper anti-coagulated. So don’t forget to check the coags. Most often LVADS are placed for significant heart failure, or as a temporizing measure while the heart function heals or as the patient awaits a transplant- that means that these patients will have some structural heart abnormalities and therefore will be at higher risk for arrhythmias… Get an EKG! Bedside ECHO if capable is going to be super helpful so start getting ready to take a look at some function and ventricles.
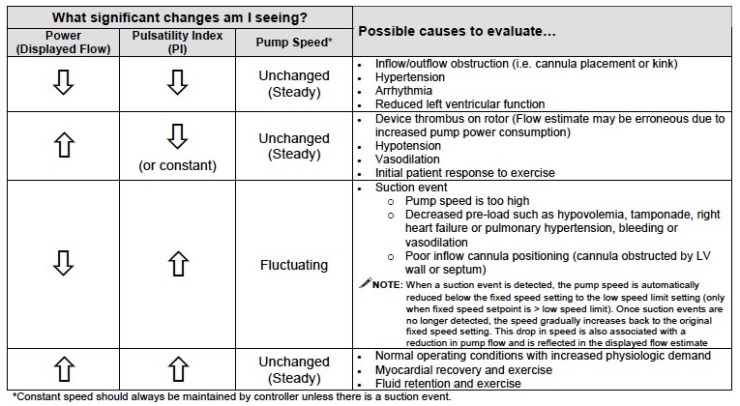
Oddly enough, you should also actually check the device. Make sure the batteries have charge, that all the lines appear connected. That the drive line (the line that runs from the external controller to the actual implanted device) is not kinked or cut. The controller itself may be flashing a message at you or it may just be showing its parameters. 4 main things to look at will be speed (set according to ECHO results), Flow (calculated with math), Power (this is the average required power over a cardiac cycle), and Pulsatile Index (how much output is being provided by the still beating heart v. the pump)
Emergencies
Hemodynamic Complications
So like I said before, the bit in the Left ventricle is the sucking bit. Which means that it needs blood, and plenty of it, in the ventricle in order to function. AKA the device is Preload dependent. No one will blame you for giving the patient fluids. Help that preload out! You may see evidence of low preload on your ECHO with a small RV. Also, the controller may be warning you of “low Flow.” Otherwise, look at your patient… do they look fluid down? This is a common mishap as these patients with significant heart failure have been previously living with physicians always telling them to cut back on fluid intake… This issue has an easy answer- give them fluids.
While on the topic of perfusion we cannot forget that these devices are also afterload sensitive. The motor needs to fight against all the systemic resistance in the body to push the blood along. This is why there is such a strict MAP cap (90). When the pump has to work hard to overcome the afterload, the increased work can lead to thrombus formation. (see below!) The device might read low power, low PI. Remember that you can always give vasodilators to decrease the afterload.
Suction Event
In the event of a suction event, the machine may read low Power, high PI. The pump speed may automatically fluctuate. A few common causes of suction events include hypovolemia, malpositioning, poor RV function( tamponade, dysrthymia, etc.). Basically the machine is attempting to suck blood from a dry ventricle and instead suction-cups the ventricular septum. You can do a few things here: give fluid, slow down the speed of the pump. This allows time for the ventricle to relax and fill.
Thrombosis

Some signs that there might be thrombosis in the device include high power, heat of the actual device, ECHO with increasing LV dimension in diastole (aka device not able to suck the blood forward as well) and increased frequency of aortic valve opening. If you are not positive, and the patient is stable- you can obtain a CT scan with contrast to assess for clot. But you might want to talk to your radiologist prior to ordering so that you get the right protocol. Further evidence of thrombosis is elevated LDH (LDH > 1150) – this comes from hemolysis within the thrombosed pump. (Zoler, 2016) Along the same lines- as the motor chops away at this clot it can send small emboli along the body… so be wary of this in an LVAD patient presenting with stroke signs, altered Mental Status, etc. Despite significant anti-coagulation about 2-13% of LVAD patients experience thrombosis… usually at about 1 year after implantation. (Nair et al 2016) So definitely don’t forget this.
First things first. Start them on as much blood thinners as you can, I.E. Heparin drip, antiplatelets. Consider sending decompensating patient directly to LVAD exchange or catheter directed thrombolysis. If these are not available AND patient is not responding to the anticoagulation AND they have no contraindications – then you can consider TPA.
Bleeding
Now for the exact opposite and the most likely complaint you will see from an LVAD patient. Bleeding. This can be any bleed. Epistaxis, Intracranial, GI. Whatever can bleed, will bleed. Not only are these patients at high risk of bleeding from their home anticoagulation (typically Warfarin) but they also may develop von Willebrand Disease from shearing forces of the pump. AV malformations in the GI tract may worsen without a pulsatile flow, liver failure from congestion from heart failure definitely won’t help. Whatchu do? Reverse it. This will likely need to be a conversation with their VAD coordinator- but you may be able to reverse their anticoagulation. If the bleed itself is life threatening, you can also consider the big anti-bleed guns (TXA, PCC, FFP, etc.)
Arrhythmia
Arrhythmia may be one of the most difficult words for me to spell. It is also very common in these patients. Treat these like you would treat them in a non-LVAD patient. That’s right – Afib? Rate control! Unstable VTach? Shock! I know they have metal in their chest but as we’ve discussed- the device is preload dependent. So the heart needs to function enough to bring blood to the device or else the device won’t be able to do it’s job. So you gotta get the heart back first and foremost.
Now for a related and more debated topic… CPR? The concern is that compressions may dislodge the device and cause significant harm. But from evidence of some light reading: most opinions lead towards pro-CPR. If the heart and the pump aint working then there is no other way to perfuse the brain. BUT this is still super controversial at this time. Some people suggest abdominal compressions, some people say to jump straight to ECMO. Use your clinical judgement, talk to some friends, and patiently wait for more data…
Conclusion
These are sick patients. Not everything they come to your department for will be LVAD related. Buuuut it is good to brush up on how they function and what are common issues so that you don’t miss some of these hard hitter emergencies. Golden Nugget- call their device coordinator and let them help you troubleshoot while you scan for other issues.
Citations
- Isakson, B. C. Lu, K, Singh, M. Holtz, M. Young, N, Ostermeyer, D. Donaldson, R. Left ventricular assist device WikiEM, Published on 9.25.2019. Accessed on 10.31.2019. Available at [https://wikem.org/wiki/Left_ventricular_assist_device#cite_note-9.]
- Nair N et al. Thrombolytics in VAD management — A single-center experience. Int J Cardiol Heart Vasc. 2016 Jun; 11: 49–54.
- Nickson, C. Ventricular Assist Device (VAD) Life in the Fastlane. Published on 9.14.2019. Accessed 10.31.2019. Available at [https://litfl.com/ventricular-assist-device-vad/]
- Weingart, S. Left Ventricular Assist Devices (LVADS). EMCrit Blog. Published on July 8, 2012. Accessed on October 29th 2019. Available at [https://emcrit.org/emcrit/left-ventricular-assist-devices-lvads-2/].
- Zoler ML. Cardiology News. STS: Lactate dehydrogenase of 1,150 IU/L flags LVAD thrombosis. Published Feb 19, 2016. Accessed on 10.31.2019. Available at [https://www.mdedge.com/ecardiologynews/article/106621/heart-failure/sts-lactate-dehydrogenase-1150-iu/l-flags-lvad]