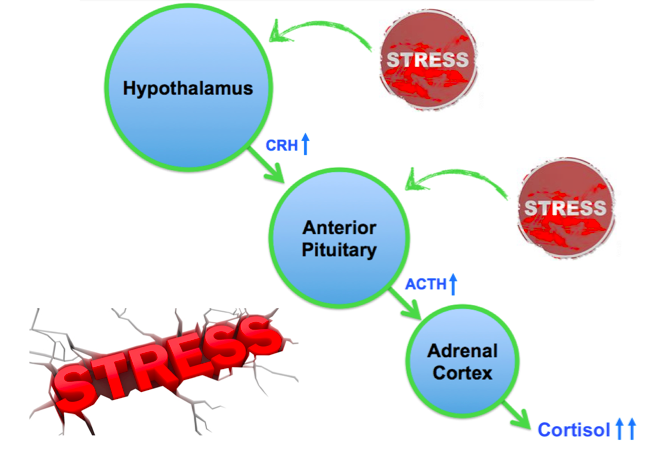
So the adrenal gland is the little cap on top of the kidney. It is broken up into two parts- the medulla and the cortex. For now, lets ignore the medulla and focus on the three parts of the cortex. Since we aren’t studying for step II I don’t really care what hormones come from which part- but it is important to remember that mineralocorticoids, corticosteroids and androgens are all released from the cortex. In a typical day the body will release these in response to stress through the HPA axis.
Etiologies
Adrenal Crisis comes about when someone with an underlying adrenal insufficiency undergoes a period of severe stress. The body tries to react to it, but the adrenal gland has nothing left to give. These episodes of stress can vary from trauma, to surgery, to dehydration or even emotional stress. (Hahner et al.)
The underlying insufficiency can be primary (coming from the adrenal gland itself) or secondary (coming from further up in the HPA axis.) Examples of primary insufficiencies include Addison’s disease; this is an auto-immune destruction of the adrenal gland resulting in the typical findings of skin hyperpigmentation, Waterhouse-friedrichson; this is a hemorrhagic mauling of the adrenal gland secondary to meningococcemia, infections; specifically infections such as TB or HIV, and tumors. Secondary insufficiencies include pituitary apoplexy, pituitary tumors, and one that needs a little expanding upon: chronic steroid therapy.
This is one of the main reason’s why we don’t want to give steroids to people long term. However, this has been found to be the etiology of adrenal insufficiency even in people receiving joint injections of steroids or even inhaled steroids. So getting a good history can be really important here.
Presentation
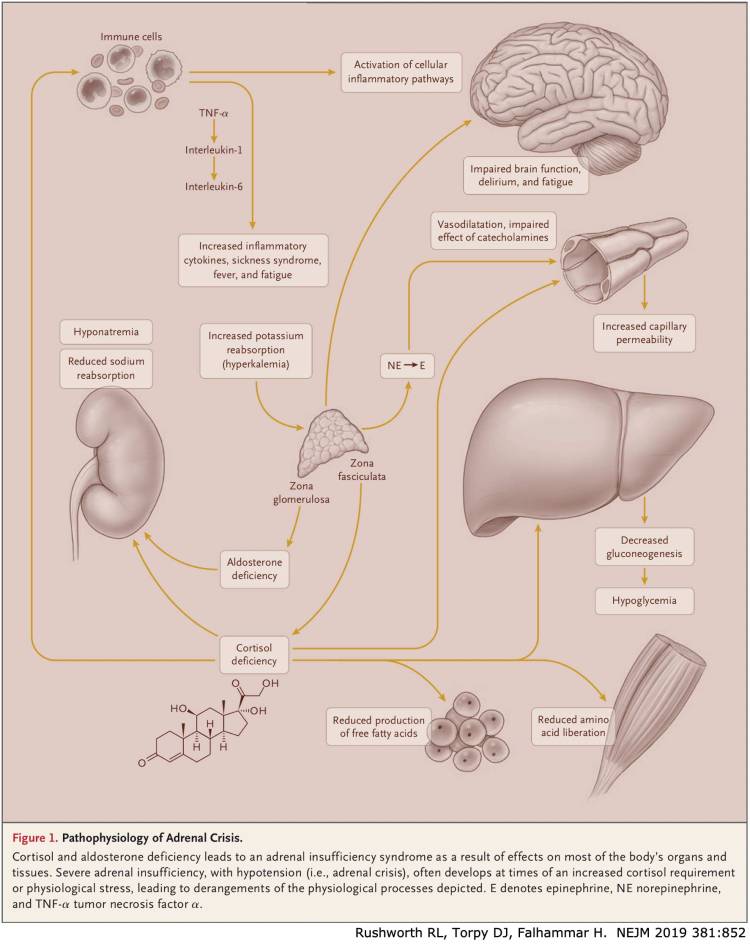
Basically people in adrenal crisis can present with any chief complaint. They may have pains, infections, weakness, confusion, skin changes. The big kicker to this, is that they will look sick. Their pressures will be low and will stay low in spite of your iv fluid resuscitation. Normally cortisol has an additive effect with catecholamines to vasoconstrict… now, however without enough cortisol vasodilation will reign.

Their labs will come back all a-kilter as well.
- Hypoglycemia: cortisol is a catabolic hormone. So typically in times of stress it will instruct the liver to perform gluconeogenesis. Without enough cortisol, comes not enough sugars.
- Hyponatremia: Aldosterone (one of the mineralocorticoids) is now lacking. So instead your kidney is wasting sodium.
- Hyperkalemia: the deficiency of aldosterone instructs your kidney to retain the positively charged ions as well. So you keep extra potassiums.
- Non-anion gap Metabolic Acidosis: Again coming from the kidney, those small H+ ions are being kept, leading to acidosis.
- Elevated BUN and Cr: this actually has nothing to do with the aldosterone deficiency and everything to do with the hypotension. This is a pre-renal AKI.
Whaddya gonna do about it?
We are going to be sending a lot of labs on these patients, go ahead and treat them like a septic patient (especially as the crisis can be onset by infection!) That means go ahead with the cultures and 30cc/kg fluid resuscitation. What I would change however, is the fluid itself. If the patient is severely hypoglycemic, go ahead and alter the fluids to D5NS and check the sugar every hour. Oh, and if they need it, start pressors early.
Now this is where the treatment will start to vary.
If this patient says- hey, I’ve got the Addison’s disease, or their chart says “hx of Adrenal crisis” and so you know that this is likely an Adrenal Crisis. Then you given them Hydrocortisone bolus (100mg IV) and get them up to the ICU.
If this is looking like it might be a crisis, but there is no history. Then instead of the Hydrocortisone you should consider Dexamethasone 4mg IV. The reason why, is because the Dexamethasone will not block or alter the ACTH stimulation test that they will want to do upstairs to assess for adrenal insufficiency. Otherwise, the hydrocortisone will not be harmful for them, so if it’s all you got, that is a-okay.
As for the electrolyte and kidney disturbances, this should change by itself with the steroids and all the crystalloid. However, as it acutely endangers the heart, you can also give your typical hyperkalemia treatment.
Prevention
Now, I thought this was really interesting. But if you see a patient in the ED under stress ( a trauma, a gastroenteritis) and they have a history of adrenal insufficiency- you can consider starting them on PO steroids for home, or even IV and have a low threshold to admit. This can help prevent them from going in to crisis!
Citations
- Arlt, W. Society for endocrinology Endocrine Emergency Guidance: Emergency management of acute adrenal insufficiency (adrenal crisis) in adult patients. Endocrine connections. Volume 5 (5) September 2016.; G1-G5
- Cloyd, T. Core EM: Adrenal Crisis. Published: December 2015. Accessed March 2020. <https://coreem.net/core/adrenal-crisis/>
- Farkas, J. Adrenal Crisis. Published February 2017. Accessed MArch 2020. <https://emcrit.org/ibcc/adrenal-crisis/>
- Stefanie Hahner, Christina Spinnler, Martin Fassnacht, Stephanie Burger-Stritt, Katharina Lang, Danijela Milovanovic, Felix Beuschlein, Holger S. Willenberg, Marcus Quinkler, Bruno Allolio, High Incidence of Adrenal Crisis in Educated Patients With Chronic Adrenal Insufficiency: A Prospective Study, The Journal of Clinical Endocrinology & Metabolism, Volume 100, (2), 1 February 2015,; 407–416,